


Hemsworth Labour MP Jon Trickett led a Westminster Hall debate this morning on health inequalities and the COVID-19 outbreak in West Yorkshire. The left-winger challenged the government to do more to get a handle on the comparatively high rate of infection in his home county and noted how the rate there declined far more slowly than the national average after the vaccine was diverted away from Yorkshire on 11 February.
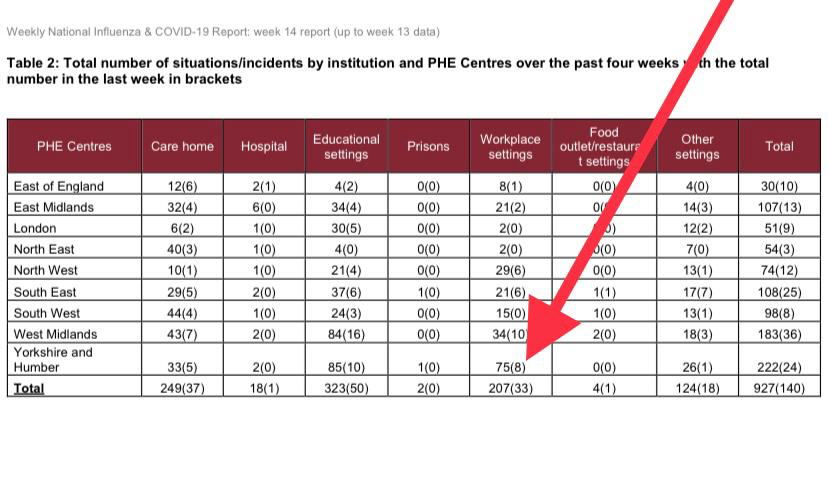
Trickett highlighted the latest Public Health England (PHE) figures showing that in the last four weeks Yorkshire and the Humber – which has less than 10% of England’s population – accounted for 36.2% of all workplace multi-infections. He argued the occupational structure of his area meant enhanced risk of workplace infections.
The former Labour front-bencher called on the government to deploy rapid response teams to areas of high infection so that local health groups (CCGs) and local authorities can tailor their response more effectively.
Trickett said:
It is completely unacceptable that once again the government’s decisions are based on what is happening in the south of the country, when up here in Yorkshire the infection rates are still raging. I demand that the government takes immediate action to correct this injustice.
There is a class dimension to this, as well as a regional one. It is the low paid working class who are most exposed by the government’s failures.
1. It is possible to note that now the vaccine was diverted that my area’s CV19 rate declined much more slowly than other areas. Indeed, in the medium term it continued to rise. More than 762 people in Wakefield have now lost their lives, a figure above the average for local authorities. The levels of vaccination in my ward are progressing much slower down the age structure in comparison to the Health Secretary or Health Minister.
2. The occupational structure of red wall areas, and Yorkshire in particular meant enhanced risk of workplace infections. In the 4 weeks to date, Yorkshire & Humber accounted for 36.2% of all workplace multi-infections (PHE). The work from home data (ONS) shows that manual, semi-skilled and front facing roles tend to have higher levels of working on site. Professional classes & the hospitality sector had higher levels of work from home, and furlough respectively.
3. In comparison to the Health Secretary and Health Minister’s area of West Suffolk, my area of Wakefield is currently experiencing nine times higher levels of infections, and indeed in one instance a ward has 1,700% higher rates of CV19.
4. Lastly, there is a strong argument that existing inequalities exacerbated by austerity, and the north south divide have made matters worse. In Yorkshire, especially rural areas, access to critical care beds is much lower. There is no doubt that the 21,000 beds axed since 2010, the 100 NHS Walk In Centres closing and the 25 A&E ward closures have made matters worse.
In today’s Westminster Hall debate, I proposed a policy to deploy rapid response teams to areas of high infection so that local health groups (CCGs) can tailor their response more effectively. The vaccine in itself is no panacea to this pandemic. It will continue to pose risks to my community and others. This would be one tool to tackle this more effectively.
Watch Trickett’s speech below:
The 7 day rate for Matt Hancock’s West Suffolk constituency is 8.4, while the rate for Boris Johnson’s Hillingdon is 36. The average for England is 27.9.
Wakefield’s is 84.
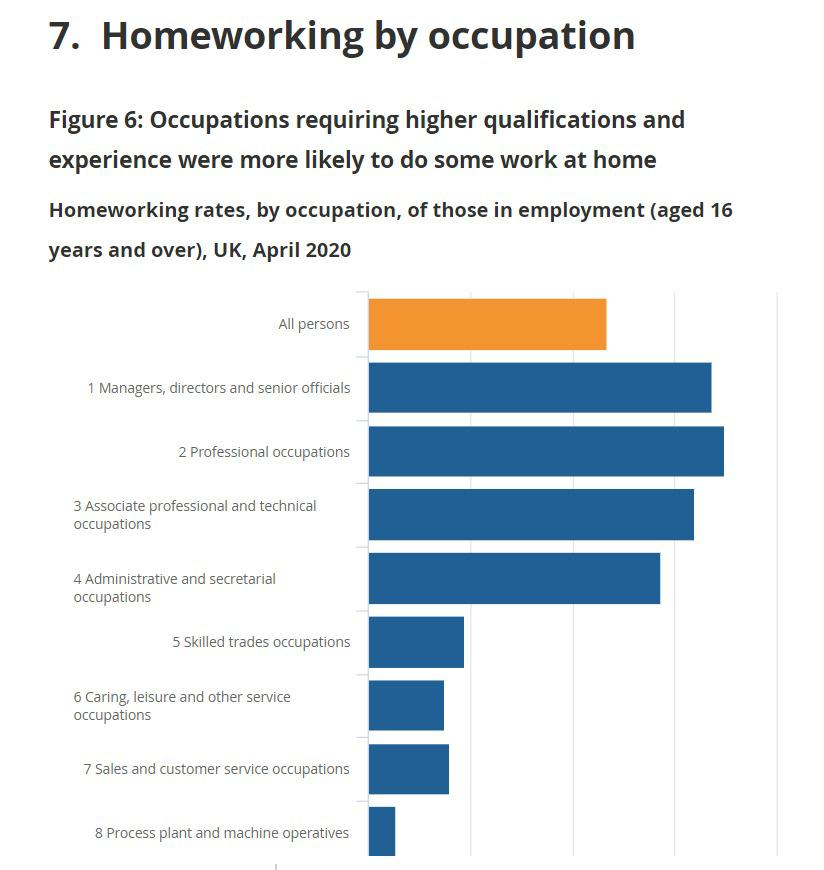
There are also significant class and regional differences in the number of people able to work from home and reduce the chance of infection:
- Professional occupations working 69.6%
- Managers, directors and senior officials 67.3%
- Caring, leisure and other services 14.9%
- Process plant and machine operatives (5.4%).
Regions
Yorkshire – 37.6%
UK – 46.6%
London – 57.2%
East – 47.3%
Workplace infections
The SKWAWKBOX needs your help. The site is provided free of charge but depends on the support of its readers to be viable. If you can afford to without hardship, please click here to arrange a one-off or modest monthly donation via PayPal or here to set up a monthly donation via GoCardless (SKWAWKBOX will contact you to confirm the GoCardless amount). Thanks for your solidarity so SKWAWKBOX can keep bringing you information the Establishment would prefer you not to know about.
If you wish to republish this post for non-commercial use, you are welcome to do so – see here for more.
Got an invitation letter for a needle on 22nd February telling me as a carer for me dad I was eligible.
No stations on the Wirral doing the jabs. Nearest one was Aintree racecourse…Try again in a few days because new locations are opening up all the time.
Come the beginning of the month – Still nothing this side of the Mersey, so I rang 119 on April 2nd. They said the procedure had changed 31st March and I had to ring my GP.
Rang GP….Waiting on delivery…Try again tomorrow.
Tried again next day – Different receptionist….”You’re not on our list” she told me.
Explained that I should be…That I’d been waiting five weeks, and that 119 had told me to go through GP surgery.
Ok,I’ll put you on our list; expect a call/letter within a few days”
Heard sod-all in the almost three weeks since. I’ll be 50 on the 6th of next month. Maybe they’ll invite me then.
Ring them and ask if they’ve got the vaccine in yet. If you’re flexible, tell them you can come any time if they get a cancellation. Got mine that way.
*April 1st, not 2nd.
Coronavirus is a virus that feeds on inequality. The government’s Pandemic Management is a policy which worsens both inequality and absolute poverty AND the threat of the pandemic..
* Ineffective Testing using non-diagnostic PCR tools to intentionally mis-test when undertaken at the wrong amplification levels (which the |UK Gov did until end-Jan this year and was publicly censored by WHO for);
* Inappropriate Isolation policies that disincentive precarious workers from participation.
* Failure to identify and concentrate on the demographic groups most vulnerable to SARS-CoV-2 infection.
* A narrative which intentionally fails to disclose the whos, whens, hows and whys of Covid-19 Infection/Fatality rates.
* Dangerous promotion of experimental mRNA gene therapy which is still under-development (until Nov 2022at the earliest) and cannot therefore be described as “safe” or even “effective” – remember, the testing phase of, for example, the Oxford/AZ ‘vaccine’ does not end until Nov 2022 or later.
The Billionaire-class is the only beneficiary of this Government’s criminally bad “pandemic management”. The rest of us are its victims, its objects – and we WILL pay the price, several times.
Covid has exposed the hidden cost of a neoliberal society. Poverty, the shocking prevalence of chronic illness/physical disabilities and the truly awful mental health of large sections of the community have come home to roost.
What we can expect from future governments of any persuasion is less, not more. It’s time that statisticians worked out the price of neoliberalism.
Yes and also:
WHY (according to WHO Covid Dashboard in Feb2021) had FORTY THREE percent (43%) of global COVID deaths occurred in only TWO countries which together comprise just under FIVE percent of the world’s population?
The two counties were UK and USA – a petri dish of extreme neoliberalism and the good ol’ USA.
Neoliberalism causes government, media and the billionaires to watch each others’ backs and is, I would say, a major facto in the UK’s atrocious pandemic management.
Remember, the infection fatality rate if SARS-CoV-2 is cica 0.33 % atm, (look it up) but you’d never think so if you depended on the BBC and MSM for your news and information.