
I’ve written briefly about the FOI information I received from the excellent South Tees Hospitals NHS Trust regarding plans for staffing cuts. While this did not reflect such a bad situation as is currently being experienced by NHS workers in the South-West, who are facing attempts from a legalised cartel to coerce them into worsened conditions and pay, it did demonstrate very clearly how the government is trying to set up the NHS to fail by overstretching already thin resources, as an excuse for faster and more extensive privatisation.
Since I wrote that post, I’ve received some additional information, from an NHS staff nurse (@archangelolill on Twitter), about the implications of the specific measures STHNHST is being forced to undertake because of the Coalition’s ‘efficiency’ drive, and which show even more clearly the ways in which these measures are overstretching even the dedicated, professional people who staff our NHS hospitals and other facilities. We’ll look in some more detail at the specific cuts and extensions, and what they mean. FIrst, here’s the table that the Trust sent me again:
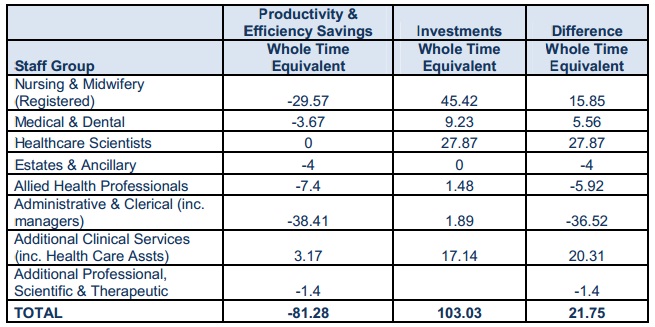
And the clarifications that they provided on request:
1) The majority of the reductions in Admin & Clerical Staff (Including Managers) have been
identified from corporate areas and will be met through natural wastage. Management
restructures and administration reviews in clinical areas account for the remainder identified as
a result of planned retirements and anticipated resignations from staff again through natural
wastage.
2) Investments include the development of specialist services such as Cancer, Neurosciences and
Cardiothoracics as well as developing Trauma services after being designated as a Level 1
Trauma Centre.
So, what does this information mean?
Reduction of 36.52 ‘admin,clerical & managerial’
While a non-specified majority are said to come from ‘corporate’ functions, the balance comes from ‘Management restructures and administration reviews in clinical areas‘. This will include functions such as ward clerks. Ward clerks may seem like an unglamorous clerical function, and they’re not usually the target of appreciation by grateful relatives that nurses can sometimes be. However, on a ward without a ward clerk, nurses have to spend time answering phones, doing time consuming discharge paperwork, patient review appointments etc that could otherwise be spent caring for patients.
This makes complaints about care standards more likely, which suits the government’s purpose of justifying privatisation – and also endangers lives. Paperwork etc might be done incorrectly, so that a patient receives the wrong drugs or doesn’t receive the right ones, or overstretched nurses might miss a key sign that a patient is about to take a turn for the worse. My wife has told me of numerous occasions where she or a colleague has spotted some subtle sign that a patient was about to go into cardiac or respiratory arrest – and how proud they’ve been to have done so when they were rushed off their feet. Placing an increased clerical burden on nurses makes such ‘saves’ far less likely.
Increase of 15.85 nurses
While this increase may appear positive, if nurses are taking on extra clerical tasks the headline increase is already misleading. Add to this the fact that major additional services are going to be provided from a nursing resource that is increased only fractionally, and the news is anything but good.
Care-intensive new services
The proposed new cardiothorasic, neuroscience and cancer services are care intensive and generally require a high nurse-patient ratio – far more than the proposed increase to nursing staff across the whole hospital of only 15.85. Staffing these areas properly will entail moving staff away from existing wards and functions – which again signals the government’s intention of spreading resources so thinly that services malfunction or even collapse, so that the government can then come in to ‘save’ hospitals and patients as cover for privatisation.
Increase of 20.31 for ‘additional clinical services/healthcare assistants
From the table, it looks like these additional carers will be allocated to areas where existing trained staff used to work but are now earmarked for transfer to the newly proposed service areas.If so the current services will be staffed with fewer trained Staff nurses and more care assistants which is bound to impact on care.Too few mentors drive care standards down as inexperienced staff are not familiar with prioritisation and patient care suffers.
Healthcare scientists: increase of 27.87
These appear to be destined for the newly proposed services – but will be technicians with procedural involvement but not delivering patient care.
Trauma service Level 1
Trauma centers are extremely care-intensive. For example, a patient may remain in A&E for hours after
resuscitation while they are stabilised.
Other implications
One aspect that managers rarely cater for when calculating staff requirements and skill mix is the time required for dealing with distraught family/friends of patients. This never features as an objective with outcomes and measurements, and so is rarely considered when preparing staffing levels.
Trauma centers deal with sudden and unpredictable minor to fatal conditions of patients who present in acute setting, and where the most distraught & terrified family/friends are to be found. It’s therefore extremely important that staff numbers and mix are correct for this ‘front line’ of hospital care which can be a horrendous place to work or be a patient when poorly resourced.
Here’s the closing statement that my contact wrote when she sent me her information:
‘I have spent considerable time looking at the figures against the proposed services and their current services. Nurses will be stretched beyond coping & new care assistants working with fewer mentors will
struggle.
The care of the currently catered for patients will be compromised for sake of the flagship proposed services. Proposed services are of course important but they are the services that “look good”and impress. They are the headline grabbers unlike equally important care of older people, chronically sick, general medicine and it may be these areas where nursing expertise will be diluted. And if so all you have is immoral unfair cosmetic exercise. A well-painted front door can be so very misleading!’
Of course, this is just one Trust among many. Each Trust will have its own specific story, and some will be worse than this one. But if, as I would assert because I think the facts demand it, the plans South Tees Trust is being forced to implement are a symptom of the government’s very intentional plan, then it’s very evident that the aim is (at least) two-fold:
1) to degrade NHS care so that the NHS can be attacked in the public mind and more rapidly privatised.
2) to force Trusts to add new services with no increase in overall investment. This allows the government to trumpet the ‘improvements’ and ‘efficiencies’ that it’s ‘reform’ of the NHS is creating, while simultaneously creating an over-stretch that will lead to worse care, increased complaints and even patient deaths that will contribute to aim number 1.
The government is cynically gambling with people’s lives for its own ends. If it is allowed to continue with its plan, there is no doubt at all that people will die unnecessarily as a result. I hope it isn’t you, me or one of our loved ones.
If you would like to add your voice to the resistance to the coalition’s dismantling of our National Health Service, please sign the petition linked below and circulate it to as many people as possible to do the same. Achieving a repeal of the NHS Act may not be possible during this Parliament, but the louder the voice of those who believe the Tories’ ‘reforms’ are a calculated evil, the more ammunition the resisters will have – and the clearer will be the call on the next government to reverse the changes. And if, like me, these facts outrage you, find out what’s going on locally and nationally that you can support, and get stuck in!
http://www.gopetition.com/petitions/petition-to-repeal-the-health-social-care-act-nhs-a.html
Signed!
“The government is cynically gambling with people’s lives for its own ends. If it is allowed to continue with its plan, there is no doubt at all that people will die unnecessarily as a result. I hope it isn’t you, me or one of our loved ones”
I think the military already know this. As you say, cutting an admin post then using front line staff to do the job is a complete waste of resources.
One thing that puzzled me recently about the NHS in general was is the fact that the patients’ chart format varies from hospital to hospital. For something that is a bit critical for patient care, I would have thought they would have been the same. I wonder what else could cause confusion?